 A hip dislocation is a devastating injury…
A hip dislocation is a devastating injury…
Late in the 2019 collegiate football season, Tua Tagovailoa, Alabama’s star quarterback, projected to be the first pick in the 2020 NFL draft, was sacked while playing Mississippi State and sustained a violent injury to his right hip. After being carted off the field, he was diagnosed with a hip dislocation and a fracture of the posterior wall of the hip socket.
Whereas, I don’t have any direct information about the specifics of his particular injury or surgery, This is a good example to initiate a discussion of this particular injury. So let’s take a closer look at this rare but serious injury.
What is a hip dislocation?
A dislocation is a complete disruption of a joint. A normal joint involves two or more bones that are held together by the shape of the bones, the ligaments, firm bands that attach to each bone, and the surrounding muscles. Different joints have different degrees of stability. The greater the stability, the less likely a disruption. When there is a disruption in which the bones are completely separated from one another, that is called a dislocation. Subluxations, on the other hand, are only partial separations. Dislocations can occur at any joint. Some joints, however, are more susceptible to dislocations than others.
What is the important hip anatomy?
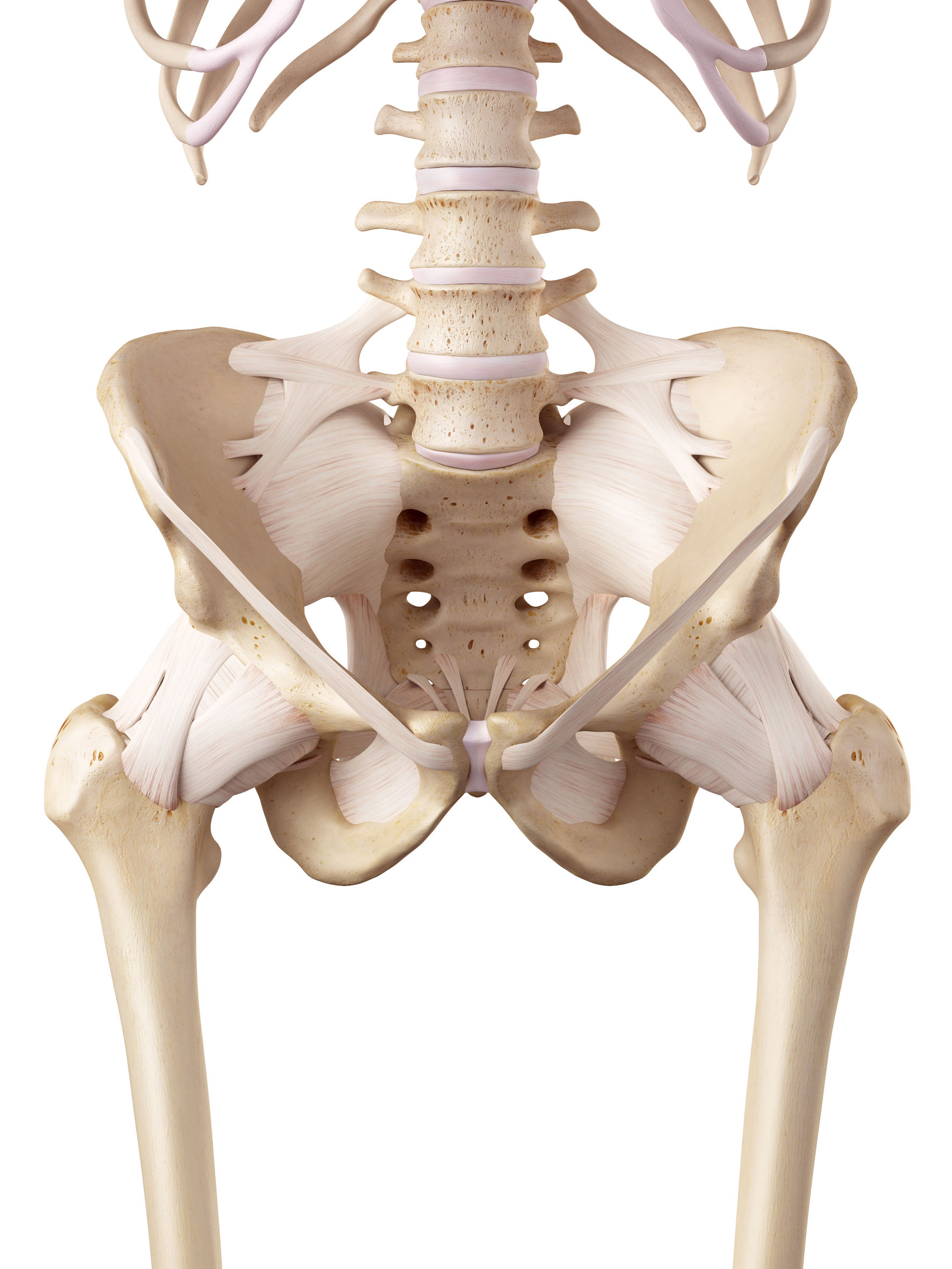
Drawing of the hip joints with overlying ligaments
Our hip joint is a ball and socket joint and is one of our most stable joints. This makes sense. We must walk on this joint, moving in many different directions and often changing that direction abruptly. This would not be possible with a less stable joint. So fortunately for us, as we have evolved to upright walkers, our hip joint has become increasingly stable.
The stability of our hip joint results from several unique characteristics. Most importantly, the top of our femur, our femoral head (the ball), sits deeply in our acetabulum (cup). Further stability results from extremely strong ligaments running from each bone to the other. Additionally, we have a thick soft cartilage tissue called the labrum running along the acetabular rim. This is not only a firm attachment for many of the hip’s ligaments but it also provides a seal to our hip joint adding even further stability. Finally, we have very large and strong muscles that surround our hip. These add dynamic stability as we use our hip.
How does a hip dislocation occur?
There are two main types of hip dislocations. The less common is an anterior dislocation. An anterior dislocation occurs when the femoral head dislocates and rests in front of the acetabulum. A posterior dislocation, by far the more common of the two types, is a dislocation in which the femoral head ends resting on the backside of the acetabulum.
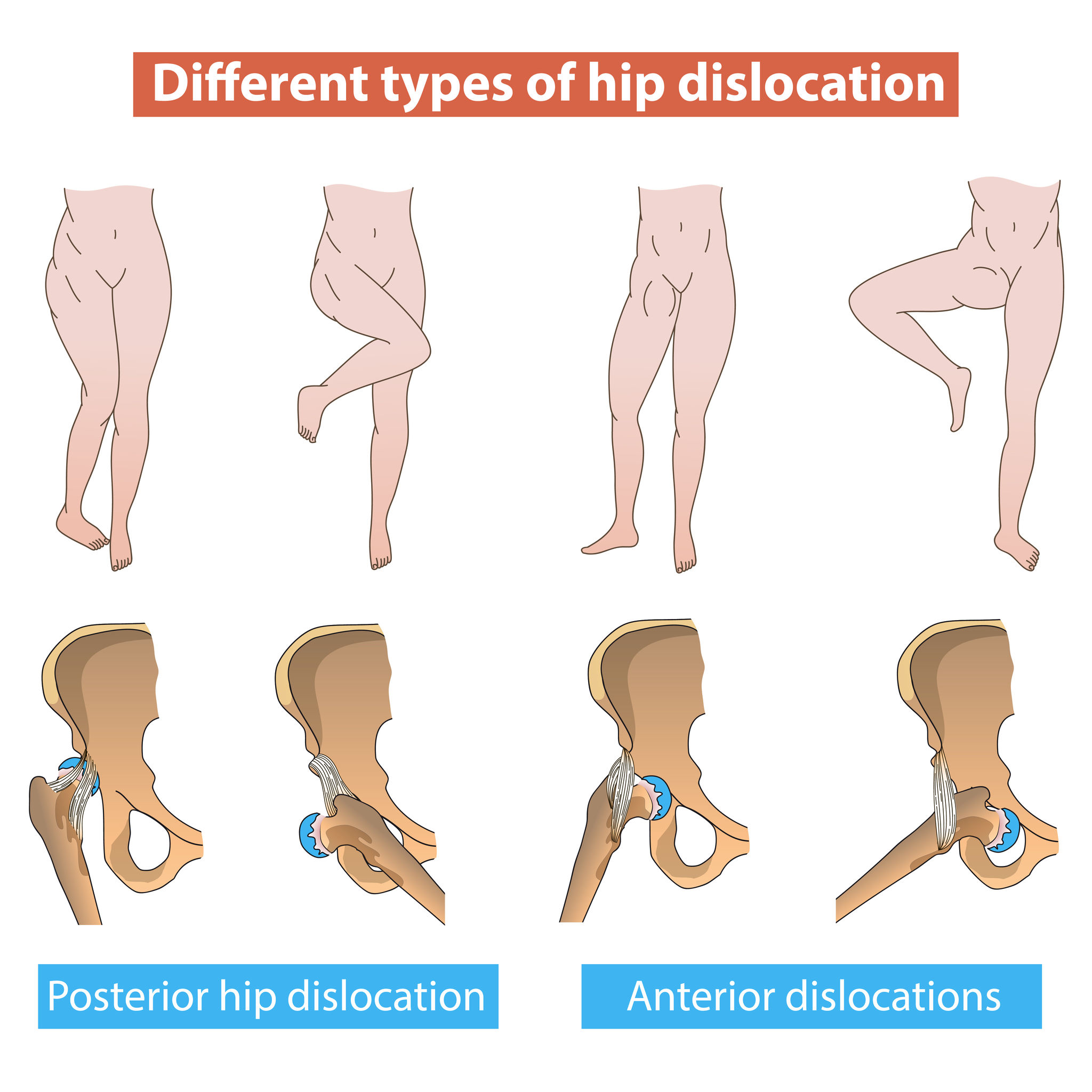
Anterior and posterior hip dislocation
The type of dislocation is determined by the direction of the force on the limb and the position of the hip at the time of injury. The most common mechanism of injury causing a hip dislocation is a motor vehicle accident sustained by someone inside the car. Other common mechanisms are falls from a height and athletic injuries, as was the case in Tua’s injury.
Most dislocations occur with the hip in flexion to approximately 90 degrees along with what is called adduction (the leg is close to your midline). In this position, the hip joint then sustains a force directed from the knee, along the thigh, towards the hip. This is a common mechanism occurring in someone inside a car that strikes their knee against the dashboard as a result of an accident. This also is a common mechanism in an athlete that lands hard on their knee.
Why is a hip dislocation so bad?
Because the hip joint is inherently stable, it requires significant force to overcome the stabilizing structures and dislocate the hip. As a result, there are often associated injuries seen along with hip dislocations. It is not uncommon for those sustaining a hip dislocation to also sustain a knee injury. Fractures of the thigh bone also commonly occur with hip dislocations as well.
In addition, there are often other injuries to the hip joint, itself. Fractures to the acetabulum are common. Sometimes these can be so great that stability can only be achieved by surgically securing the broken piece in place. Other times these fractures can be small. This can leave loose-bodies of bone and cartilage floating within the joint. These loose-bodies are of concern because they can be destructive to the cartilage surfaces of the joint over time – just like sand in a piston.
Additional injuries directly to the cartilage and to the labrum at the time of the injury are also common. Even injuries to the surrounding nerves can occur. These are present in as many as 15% of cases. Nerve injuries can frequently be temporary and resolve. However, in some cases, they can be permanent and catastrophic with loss of significant function and sensation of the lower leg.
Finally, the blood supply to the femoral head can be disrupted by this injury as well as by treatment and this can lead to the most common complication resulting from a hip dislocation – femoral head osteonecrosis (Osteo – bone, Necrosis – death).
What are the symptoms of a hip dislocation?
This is not a subtle injury. As mentioned, a hip dislocation requires tremendous force and is often associated with additional injuries. Therefore, when someone dislocates their hip, there will be significant pain. Furthermore, the leg will have an obvious deformity that can not easily be corrected. In posterior dislocations, the leg will be flexed at the hip and rotated inward. In anterior dislocations, the leg will be more extended and rotated outward. The person who’s hip is dislocated will not be able to bear weight. In fact, just moving will be extremely painful and so anything more than minimal leg motion will not be well tolerated. Finally, if a nerve injury has occurred, there may be a loss of function of the foot and ankle and loss of sensation of parts of the lower leg.
How are they treated?
The initial treatment is directed at making a prompt diagnosis. Confirming the diagnosis of a dislocation is critical. Fractures of the proximal femur might preclude relocating the hip by the usual mechanism of pulling on it. Often the diagnosis can be obtained with plain X-rays. On occasion, a CT scan of the hip may be beneficial to assess for fractures that aren’t displaced and therefore not easily seen on X-ray or to identify loose pieces of bone and cartilage within the joint.
Once the diagnosis is confirmed, then putting the femoral head back in the joint (“reducing“ the hip) in a timely fashion is critical. This will almost always require the assistance of anesthesia. The longer the head remains out of the joint, the more the blood supply to the head is potentially compromised and the greater the risk of the bone of the femoral head developing osteonecrosis.
After the joint is reduced, stability must be assessed. In those cases where a fracture of the acetabulum leads to persistent instability of the joint, the fracture must be fixed to stabilize the joint. If loose-bodies in the joint are identified, these must be removed with either an open or less invasive, arthroscopic procedure.
Finally, after a hip dislocation, reduction and any additional procedures performed, the hip as well as the entire lower extremity and patient, for that matter, will require extensive rehabilitation. Initial weight-bearing status is controversial, with no good data to guide whether early or delayed weight-bearing is best. Nonetheless, the rehabilitation will need to be performed slowly and progressively over an extended time period.
What is the expected outcome?
The prognosis for this serious injury is guarded. When hip dislocations occur with little or no bone fractures, they are relocated rapidly, are found to be stable, and do not require major open surgery, the results can be good in nearly half the patients.
Unfortunately, these more simple cases are rare. As mentioned above, when a hip dislocates, additional injuries to the joint cartilage as well as bony destabilizing injuries frequently occur. These put the hip at risk of developing hip arthritis in the short or long term. In fact, the likelihood of developing painful hip arthritis following a hip dislocation is relatively high, occurring nearly 25% of the time.
Even more worrisome is an injury to the blood supply of the femoral head and subsequent development of osteonecrosis. As previously mentioned, when osteonecrosis occurs, the bone of the femoral head dies. This often results in the bone collapsing. Which then frequently results In a disruption of the overlying cartilage. Together these usually end with a painful deformity of the femoral head.
Either of these outcomes can be devastating and the likelihood of developing just one of these after a hip dislocation is as high as 70%.
Both of these problems can occur rapidly or years after the injury. Either way, they almost always end with disabling pain and functional limitations even with simple walking. Often, a total hip replacement is required to relieve these symptoms. As a result, when either of these complications occurs in an athlete, it likely means an end to their competitive career.
Tua’s Recovery
As for Tua, he underwent surgery on his hip in November 2019. The surgery was performed by one of the world’s leading experts on fractures of the acetabulum, Dr. Chip Routt. His surgery was then followed by extensive rehabilitation. By all accounts, he appeared to have made an excellent recovery, On 4/23/2020, Tua was selected #5 by the Miami Dolphins in the first round of the NFL draft. Although it is still relatively early and whether or not Tua will develop late complications from this injury, is unclear. For now, things are looking good and we wish him the best going forward.